

Written by:
Colleen Bridges, M. Ed., NSCA-CPT, Parkinson’s Fitness Specialist
Dr. Caitlin Bender, OTR/L,
Betsy Lerner, MA , Parkinson’s Fitness Specialist and Rock Steady Boxing Certified
FEET! Big feet, little feet, pretty feet, gnarly feet, dancing feet…HAPPY feet! It doesn’t matter what your feet look like, what does matter is if your feet are able to support you. Did you know that by the time you are 50 years old you’ve logged approximately 75,000 miles on your feet! WHAT!!! Now, there is a great excuse for a pedicure!
AND, did you know there are no two sets of feet exactly alike? Each set of feet has its own combination of size, shape, structure, flexibility, strength, endurance, walking pattern, sensation and healing capacity. WOW!
You have 26 bones, 29 muscles, 30 ligaments and 100+ tendons in each foot that are responsible for grounding you, balancing you, and transporting you wherever you need to go. Your feet play a critical role in the overall “chain” of movement and a healthy lifestyle.
This series of articles will cover basic anatomy of the foot, foot tasks (balance, gait etc), how Parkinson’s affects your feet, how to maintain or improve foot health and finally, drills and stretches you can do anywhere, anytime!
Let’s begin with the basic anatomy of the foot.
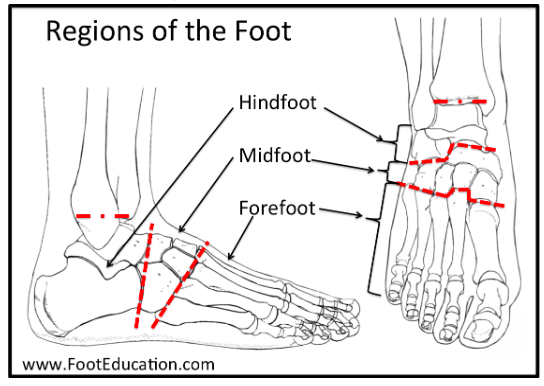
The foot is divided into 3 zones.
The Hindfoot- begins at the ankle joint and stops at the transverse tarsal joint. The bones are the talus and the calcaneus.
The Midfoot- begins at the transverse tarsal joint and ends where the metatarsals begin --at the tarsometatarsal (TMT) joint. While the midfoot has several more joints than the hindfoot, these joints have limited mobility. The five bones of the midfoot comprise the navicular, cuboid, and the three cuneiforms (medial, middle, and lateral).
The Forefoot- is composed of the metatarsals, phalanges, and sesamoids. The bones that make up the forefoot are those that are last to leave the ground during walking. There are twenty-one bones in the forefoot: five metatarsals, fourteen phalanges, and two sesamoids.
The lower leg is important to foot function and is considered the area between the knee and ankle.
The foot is a remarkable structure and is similar to a building that has two columns. The medial and lateral aspect. The medial aspect is the inside of the foot and is more mobile than the lateral aspect. The bones of the medial column include the Talus, Navicular, Medial cuneiform and the 1st Metatarsal.
The lateral aspect is the outside of the foot. It is stiffer and includes the calcaneus, cuboid, and the 4th and 5th metatarsals.

Additional areas of the foot include:
Tarsals: a group of bones that form the ankle and the back part of the foot.
Talus – the main bone in the lower part of the ankle joint. The dome-shaped top of the talus is covered with cartilage to make movements smoother.
Calcaneus – also known as the heel bone. It’s the largest bone in the foot and the foundation for all the other tarsals and metatarsals.
Cuboid, the main bone in the midfoot. It’s on the outside of the foot near the little toe. The cuboid provides stability to the outer edge of the foot, and though it doesn’t bear weight directly, it helps disperse mechanical force.
Cuneiforms – three chunky bones (medial, intermediate, lateral) that stretch in a row from the outside to the center of the foot, in line with the first, second and third metatarsals. The cuneiforms make up part of the transverse and medial longitudinal arches of the midfoot.
Navicular – a boat-shaped bone next to the cuboid bone. It connects the ankle bone to the cuboid and cuneiforms, helps stabilize the ankle and forms part of the medial longitudinal.
Front and center-front bones:
Metatarsals – five long bones, just below the phalanges or toe bones. You can usually feel these bones with your fingers. The first metatarsal connects to the big toe and is important for forward movement. The other four metatarsals provide stability to the front of the foot.
Phalanges – The 14 bones that make up the toes. The phalanges in the feet are similar to those in the hand, but they’re shorter, stronger and less mobile. The others have three – a base, shaft and head. If you’ve ever broken or stubbed a toe or have a structural issue like claw toe – common in people with rheumatoid arthritis (RA) – you know the phalanges and metatarsals are prone to injuries and other problems.
Sesamoids – two small, pea-shaped bones embedded in a tendon below the first metatarsal (closest to the big toe) on the bottom of the foot. Their job is to strengthen and reduce stress on the tendon.
Joints:
Joints are formed wherever two or more bones meet.
Each foot’s 33 joints have two essential roles: bearing weight and propelling the body forward when you’re walking or running. To do this, joints must be both stable and flexible. The foot’s flexibility comes from the large number of joints, many of which involve more than two bones.
The metatarsophalangeal joint (MCP) at the base of the big toe can be a particular problem. It briefly bears half your weight when you push off during walking, and it’s prone to osteoarthritis (OA). It’s also the most common site of gout pain, possibly because it’s far from the heart and one of the coolest parts of the body, where uric acid crystals are most likely to form.
Tendons, ligaments and muscles:
Over 100 tendons, ligaments and muscles hold the bones and joints in the foot together. Tendons attach muscles to bones; ligaments attach bones to other bones.
The plantar fascia is the foot’s longest and probably most well-known ligament. It runs along the bottom of the foot connecting the heel bone to the base of the toes. It’s made of fibrous tissue that helps support the arch. When it becomes inflamed, it can cause a deep, stabbing pain that runners, in particular, may be familiar with.
There are two kinds of muscles and tendons: extrinsic and intrinsic. Extrinsic muscles and tendons start in the lower leg, wrap around the ankle and eventually attach to the foot, fitting sort of like a sock. They allow the foot to move inward, outward and in other directions. The intrinsic muscles are confined exclusively to the foot. Most spread in layers across the bottom of the foot, where they help support the foot’s arches.
Muscles
The muscles that control the movements of the foot start in the lower leg and are attached to the bones in the foot with tendons. These are the main muscles that facilitate movement in the foot.
Tibialis posterior: the muscle that supports the arch of the foot
Tibialis anterior: the muscle that allows the foot to move up
Peroneus longus and brevis: the muscles that move the outside of the ankle
Extensors: the muscles that raise the toes when stepping (why we toe lifts every class)
Flexors: the muscles that stabilize the toes and curl them under
Nerves:
The feet also have plenty of nerves that send and receive signals from the brain and help us box, walk, jump …every movement we do in class that involves our feet.
The main nerves of the foot come off the sciatic nerve:
Tibial nerve: This nerve includes the medial plantar nerve and the lateral plantar nerve, which supply feeling to the sole of the foot. It also includes the sural nerve, which gives feeling to the outside of the foot.
Peroneal nerve: This nerve includes the deep peroneal nerve and the superficial peroneal nerve, which provide feeling to the web space between the first and second toes as well as helps the ankle move.
Saphenous nerve: This nerve branches off the femoral nerve and provides feeling to the inside of the foot.
Clearly, there is a lot involved with making sure your feet are able to move you! So much of what we do in class at Bridges for Parkinson’s starts with the feet. Why? Because your feet are the foundation of your body!
Did you know:
Your body will compensate for your weight being at the front of your feet, and cause your toes to ‘claw’ as they grip the ground or your footwear. Over time, your toes become stuck in this position, which will affect your balance.
The second change is in the length of the muscles around your ankle to cope with the shift in your weight. The changes in position mean that some muscles get stretched, while others shorten. Both of these changes alter how well you walk and mean you don’t put your heel down first as much as you used to.
The heel striking the ground is the body’s signal to the brain to generate the power to push forward. If you’re not doing this it means that your steps will be shorter, you’ll have less power to propel yourself and it will be harder to balance when standing on one leg to step the other forward.
This is why we do heel raises and hold for 5 counts followed by lifting the toes up and down (with heels up), or walking forward/backward with heels or toes up. When we are lunging or stepping, we are constantly reminding you to place your weight on the heel. And let’s not forget Fighter Tim’s “Invert/Evert” stretch at the end of class! Yes, I’m a stickler for good form to prevent injuries BUT also to remind the brain that strong gait starts with the whole foot.
So, get ready! Our awesome team of therapists and trainers are going to share vital information with you over the next few weeks about your feet! Now, go soak those feet in Epsom salt and I’ll see you in class!
References:
Manganaro D, Dollinger B, Nezwek TA, et al. Anatomy, Bony Pelvis and Lower Limb, Foot Joints. [Updated 2023 Aug 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536941/
Comments